
Introduction
Resorption of the residual alveolar ridge is an inevitable phenomenon. The morphology of the residual alveolar ridge varies from mild to excessively resorbed pattern in complete denture individuals, ultimately resulting in contrasting variations of the edentulous ridges.1 An exigent approach is generally required in cases with presence of both hard and soft tissue undercuts. These undercuts may vary from moderate to severe in form. Such conditions can affect both esthetics as well as fabrication of complete denture.2 One such example is a labially proclined maxilla with presence of an associated undercut. This may be attributed to the differential resorption pattern of the residual alveolar ridge commonly seen in maxilla than in mandible. Management of the undesirable undercuts in labial maxillary ridge may require either surgical or non-surgical correction.3 Surgical approach includes mouth preparation procedures i.e. pre-prosthetic surgery to eliminate the bulky and excessively undesirable undercuts in the labial maxillary edentulous region. This includes removal of minimal amount of bone for elimination of the undercuts. Unfortunately, use of reconstructive surgical treatment is not always feasible due to lack of patient motivation.4 Pre-prosthetic surgery is associated with decrease in the denture foundation. Systemic conditions like hypertension, uncontrolled diabetes mellitus and heart ailments further restrict the rehabilitation surgically. Moreover, some patients do not give consent for the required surgical correction. Additionally, anterior teeth arrangement becomes problematic due to limited space availability thereby bringing about unaesthetic swollen appearance of the lips.5 In such arduous situations, non-surgical treatment options include fabrication of flangeless or windowed denture, in order to restore the remaining ridges. The present article describes a simple, conservative, economical, non-surgical and non-invasive method of fabrication of windowed denture, a modification of the flangeless denture in patients with excessively bulky maxillary ridge, to provide a more pleasing & esthetically acceptable complete denture prosthesis.
Case Report
A 56 years old female patient reported to Department of Prosthodontics, with the chief complaint of previous complete dentures, being unaesthetic and even difficult insertion and removal of the prosthesis. On extra oral examination, it was found that the patient had a convex profile, ovoid face, class 2 profile, short lip length and increases mentalis muscle activity. Intraoral examination revealed that the patient had a U-shaped arch i.e. with U shaped bulky maxillary arch & V shaped mandibular arch, accompanying severe labial undercut (Figure 1).
Radiographic examination was done. All the treatment options were explained to the patient i.e. implant supported fixed or removable prosthesis and alveoloplasty followed by fabrication of conventional complete denture. Due to financial concerns, patient was not willing for implant supported fixed and removable prosthesis. Secondly, patient was a little hesitant and anxious to undergo any sorts of surgical procedure. Fabrication of complete denture was the only option left for this patient. The fabrication of the same would have resulted in an unaesthetic appearance due to excessively prominent maxillary labial flange area. Henceforth, an unconventional and modified design for complete denture fabrication was planned to meet the needs of the patient.
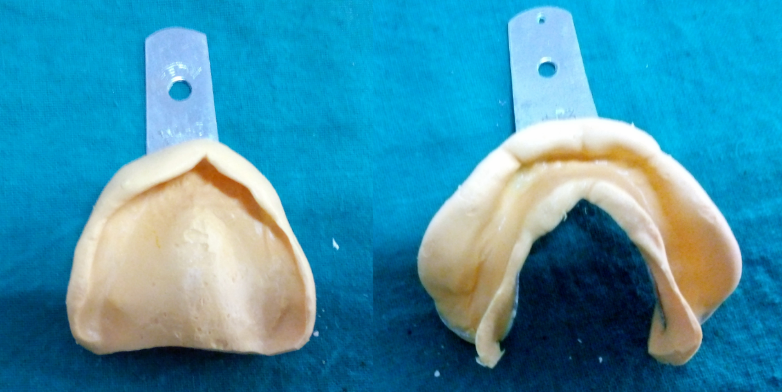
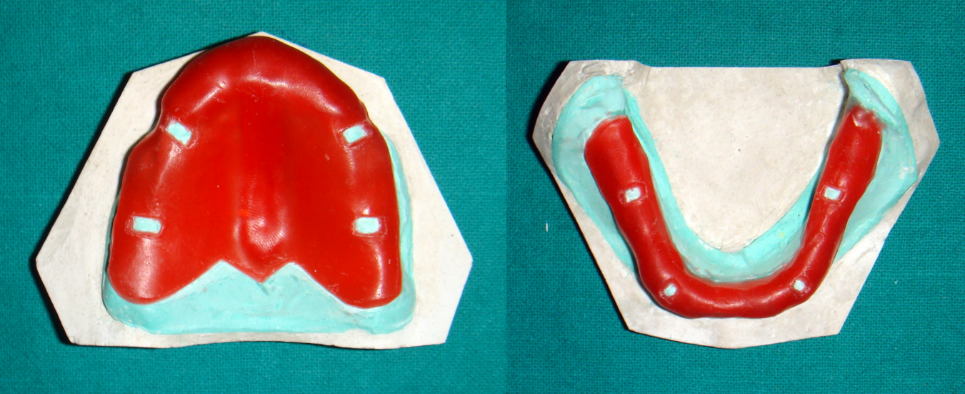
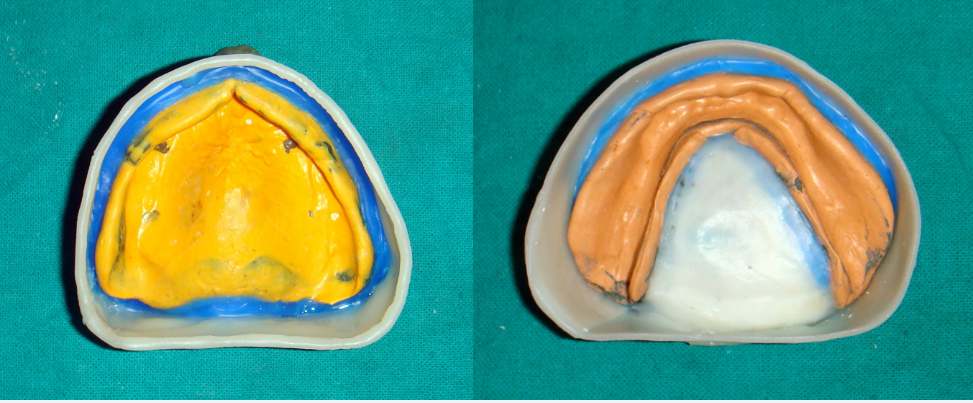
Irreversible hydrocolloid was used instead of medium fusing impression compound for preliminary impressions of the maxillary and mandibular edentulous arches (Figure 2). Wax spacer was adapted (Figure 3) over the primary cast over which the special trays were fabricated (Figure 4). Border moulding was done using low fusing green stick compound (pinnacle tracing sticks, DPI) (Figure 5) and final wash impression was done using light body polyvinyl siloxane (Aquasil ultra, DENTSPLY) (Figure 6). Beading and boxing was done (Figure 7) to obtain an accurate well-formed definitive casts (Figure 8).
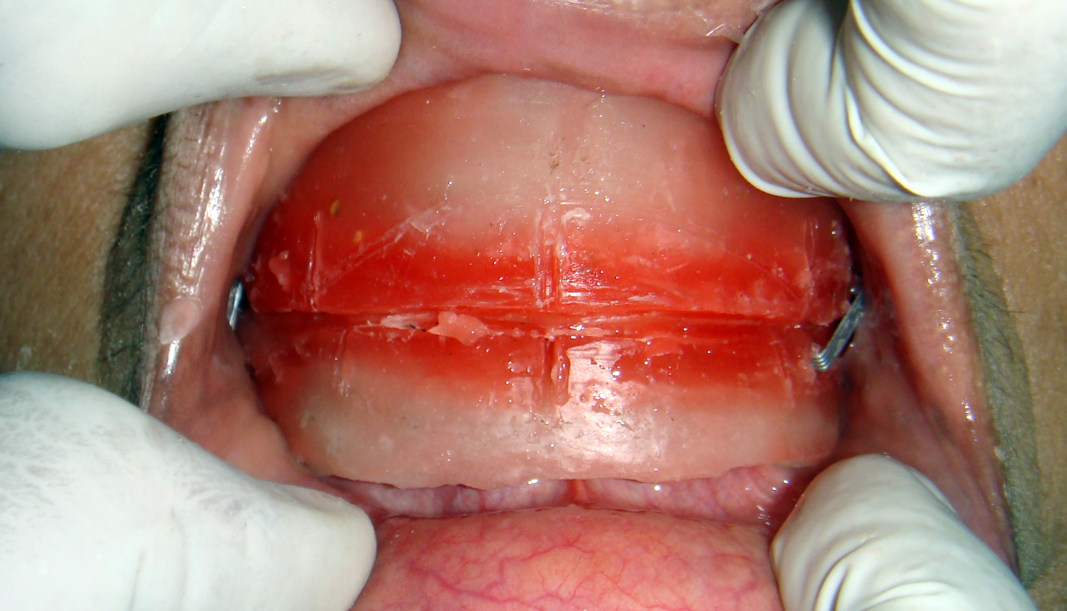
The final cast obtained was hence surveyed for identifying the undercut areas and determining the path of insertion and removal of the maxillary denture base. Temporary record base was fabricated (Figure 9) & labial flange was completely removed. Occlusal rims were fabricated followed by jaw relation records (Figure 10). Articulation was done and teeth arrangement were completed. Anterior teeth arrangement and anterior try in were done (Figure 11) initially followed by completed waxed up try in appointment. (Figure 12).
After try in, type II dental plaster was placed over the labial flange area and dewaxing procedure was performed. (Figure 13)
The procedures namely the packing and curing of heat cure acrylic resin were done in a conventional way. Once the dentures were ready, a window was created such that there was no flange on the labial aspect of the denture and the lips were in coordinate fashion with the ridge, which further reduced the labial fullness (Figure 14 & Figure 15). The borders of the denture particularly the labial flanges, were in place and sufficiently thick to provide adequate strength. The final windowed denture was finished and polished and attempted in the patient's mouth for assessment (Figure 16 & Figure 17). Occlusal corrections were done, the denture was delivered. The patient was reviewed following 1 day, 7 days and 1 month for post-insertion visits. The patient was satisfied with the esthetics, phonetics and function provided in the new set of dentures and had no difference of opinion.













Discussion
Diagnosis and treatment planning holds paramount importance in complete denture. An accurate diagnosis plays a vital role in an ideal treatment planning. Subsequently, an appropriate and accurate treatment plan reflects the success of the prosthesis. The anatomy of the residual alveolar ridges vary from individual to individual.6 Out of these, certain patients have excessively prominent and pronounced maxillary labial edentulous ridges. This may result in excessive thickness of the labial flanges, which further compromises the labial fullness as well as esthetics in complete denture that is one of the very important objectives in complete denture fabrication.7
An unconventional approach is needed for the construction of complete denture to confront such bafflement. Tissue undercuts pose a greater difficulty in fabrication of complete denture prosthesis.8 Out of these, hard tissue undercuts cause the negative effect of the retention of the prosthesis, which are obtained buccolingually and are most commonly available mechanical means of retention in completely edentulous patient. One of the conservative means to utilize the undercut includes the use of soft resilient liners that can easily adapt in the undercut area without causing any trauma to the underlying mucosa.9 Preprosthetic surgery generally decreases the denture foundation. Moreover, certain relative contraindications to the surgical modality in edentulous patient’s include uncontrolled diabetes, hypertension, and heart ailments. Modifying labial flange using surveyor helps in elimination of the undesirable undercuts and helps in determining the path of insertion and removal. One of the non-surgical approaches to preserve the ridge is known as flangeless denture.10
According to various authors, terminologies like “ridge grip esthetic prosthesis” and “gum fit dentures” have been commonly used.11 Few authors have mentioned this as “window denture" or “wing denture” to denote the removal of the labial flange in the labial frenum area and two wings show up from either side, which provides adequate space for the labial frenum.12
The present article portrays the fabrication of window denture in an excessively bulky maxillary ridge accompanied by a severe labial anterior maxillary undercut to preserve the esthetics in the patient.
Summary
This clinical report describes the fabrication of an economical, simple, quick, easy, conventional and painless method of fabrication of a window denture for rehabilitation of excessively bulky maxillary ridge accompanied with severe labial undercut. Nonsurgical procedures i.e. the prosthodontic modalities are non-invasive and can thus be utilized for the fabrication of the prosthesis for better acceptance and psychological satisfaction for the patient. The window denture was comfortable for the patient in terms of insertion, removal and function.