- Visibility 34 Views
- Downloads 6 Downloads
- DOI 10.18231/j.aprd.2020.023
-
CrossMark

Removable denture options in rehabilitation of missing dentition: A series of case reports
Introduction
Prosthetic dentistry aims in replacement of missing teeth and the contiguous tissues while maintaining proper oral functions, patients’ comfort and health and aesthetics with any artificial substitutes.[1] Prosthetic options for replacement of partially missing dentition include removable partial denture (RPD), fixed dental prosthesis (FDP), and implant‑retained prosthesis. However, FPDs or implants are opted out as treatment option in patients having excessive resorption of residual ridge following extraction and also with jaw defects following trauma or any surgery. Prosthetic rehabilitation of such cases are best carried out with conventional RPD prosthesis or fixed removable prosthesis, thus restoring the defective areas of hard and soft tissues inorder to achieve proper oral function, speech and aesthetics. Such prosthesis aims in rehabilitation with adequate stability, retention and support similar to that of a fixed dental prosthesis and better aesthetics with maintaining hygiene like that of a removable prosthesis.[2] Recently, implants have gained attention over removable prosthesis as a treatment option, yet various anatomical, physiological, psychological factors of the patients make it a contradiction. Also these are not cost effective. Conventional RPDs alongwith their various modifications are the most cost‑effective, non-invasive and comparatively better option for rehabilitation of partial edentulism. This article presents a series of case reports of rehabilitation of partial edentulism with conventional RPDs with modifications.
Case 1: Rehabilitation with tooth supported overdenture
Overdenture has always been a better treatment option as compared to a conventional RPD prosthesis. Among all practical measures used in preventive dentistry, overdenture is one of the best option which delays the process of resorption, unlike a complete denture, improves denture foundation area and increases masticatory efficiency.[3]
Case Report
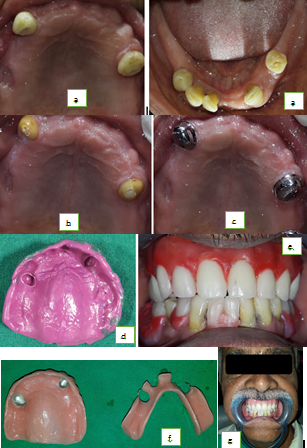
A 56-year-old male patient reported to the Department of Prosthodontics to get his missing teeth replaced. He had partially edentulous maxillary and mandibular arches. 13 and 24 were present in the upper arch [[Figure 1] a]. He was not happy with the retention of his previous maxillary removable prosthesis and wanted a new retentive prosthesis.
Treatment procedure
After assessing the inter-arch space with a tentative jaw relation of the diagnostic casts, an overdenture with long copings was suggested to the patient. For the mandibular arch, he opted for a conventional RPD. After intentional root canal of 13 and 24, teeth preparation were done and impressions made [[Figure 1]b]. The copings obtained were checked for fit in the patients’ mouth and finally cemented with glass ionomer cement [[Figure 1]c]. The thickness of the copings were not more than 1 mm. Border molding of the maxillary arch was done with green stick compound. Final impression was made with light body elastomer material (Zhermack Zetaplus) [[Figure 1]d] and master casts were poured with Type IV gypsum. Occlusal rims were made and maxilla-mandibular relations recorded intraorally. Teeth setting was evaluated in the patient’s mouth for phonetics, vertical and centric relation and aesthetics [[Figure 1]e]. The final denture was fabricated using DPI heat-cure pink acrylic resin [[Figure 1]f]. Insertion of the completed dentures were done and the patient showed satisfactory results with retention, phonetics and aesthetics [[Figure 1]g].
Case 2: Rehabilitation using precision attachment fixed removable prosthesis
Precision attachments are cost effective option for treatment as they provide better vertical support and stimulation to the underlying tissues through periodic vertical massage as compared to a conventional RPDs. They have with adequate retention and stability similar to a fixed dental prosthesis. These also help in splinting the teeth and provide favourable biomechanics.
Case Report
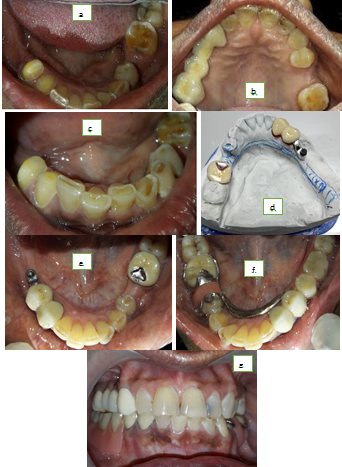
A 46 year‑old female patient reported to the Department of Prosthodontics for prosthetic rehabilitation of her missing teeth in the mandibular right posterior region. On examination, she revealed missing lower right second premolar, both first and second molars and left second premolar [[Figure 2] a]. She had missing left second premolar [[Figure 2]b] in her maxillary arch. She had a history of wearing lower removable partial denture but had a problem with retention. Considering the financial constraints, a precision attachment fixed RPD was planned for the right lower missing teeth together while replacing the left second premolar. A conventional RPD replacing the missing second premolar was planned for the maxilla.
Treatment procedure
Primary maxillary and mandibular impressions were made using irreversible hydrocolloid and casts were poured. Jaw relation was recorded and casts were articulated using facebow. These articulated casts were evaluated for interarch space and occlusion. Abutment tooth preparations were done on lower right canine and first premolar alongwith left first molar for fabrication of porcelain fused to metal restoration [[Figure 2]c]. A two-stage putty-light body impression was made of the lower arch and poured in die stone. Ball attachment was attached to a custom Ni-Cr bar in the region of first premolar. After investing and casting, intraoral framework try-in was done for proper fit and assessment of interarch space [[Figure 2]d]. The PFM crowns were cemented on the right canine and first premolar with glass ionomer cement. Similarly the PFM crown was cemented on the left first molar. Rest seats were prepared on the left first premolar and the first molar [[Figure 2]e]. A pick up impression was made with putty-light body polyvinyl siloxane material. Wax up of the lingual bar framework was done on the master cast and the final framework was cast in Co-Cr alloy. Due to very limited space for replacing the left second premolar, acrylic resin was extended from the lingual bar joining the precision attachment to close the space. [[Figure 2]f,g].
Case 3: Rehabilitation with a cast partial removable prosthesis
Removable cast partial prosthesis are considered better retentive as compared to conventional removal partial dentures. Moreover in a distal extension case, masticatory efficiency and retention with conventional prosthesis are greatly affected as a result of rotational movement around the fulcrum line. Cast partial dentures with adequate rests, tooth and tissue coverage can be a better option in such cases.
Case Report
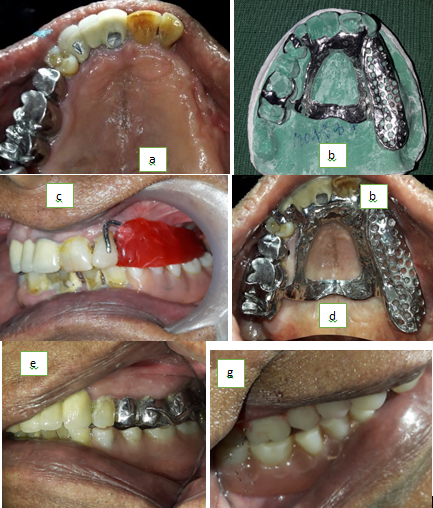
A 67 year old male patient reported with missing upper teeth. He was extremely unhappy with his existing upper RPD as it was not retentive and had chewing difficulties. Intraoral examination showed Kennedy’s Class II situation with missing left canine, premolars and molars [[Figure 3] a]. He was presented with all possible treatment modalities for prosthetic rehabilitation. He did not want implant-supported restorations considering his financial condition. He opted for cast partial denture and with his consent, the treatment was started.
Treatment procedure
Upper and lower diagnostic impressions were made with irreversible hydrocolloid and casts were poured. Surveying of diagnostic casts were done using a dental cast surveyor in which path of insertion and removal, possible interferences and guiding planes were assessed.[4], [5], [6] Anteroposterior palatal strap was planned as major connector and circumferential clasps with distal rest was planned on 16 and with mesial rest was planned on 17. On 22, I bar clasp was planned [[Figure 3]b]. Required mouth preparations were done in the patient's mouth and final impressions were made with putty and light body impression material. The casts were poured with die stone. The master cast was surveyed while blocking the unfavourable undercuts and refractory casts were made. This was followed by contouring of wax pattern. Casting and investment followed by finishing and polishing were done in a conventional manner. The metal framework was tried in the patients’ mouth for accurate adaptation [[Figure 3]c]. Occlusal rim was made and teeth setting was checked intraorally [[Figure 3]d]. Once curing was done in the conventional way, and the final prosthesis was inserted, the patient showed extreme satisfaction with both fit and aesthetics [[Figure 3]e,f]. After 1 month follow-up, the patient showed extreme satisfaction with retention and masticatory efficiency.
Discussion
The concept of conventional tooth-retained overdentures is a simple and cost effective treatment than the implant overdentures. When few teeth with good prognosis are present in an otherwise compromised dentition, they can be retained and used as abutments for overdenture fabrication, thus helping greatly in improving the retention and stability of the final prosthesis. The success of a tooth-supported overdenture treatment depends upon proper selection of case and attachments. Various factors for attachment selection like available buccolingual and inter arch space, amount of bone support, opposing dentition, clinical experience, personal preferences, maintenance problems, cost and patient’s motivation should be considered.[7]
A precision attachment prosthesis has advantages of better retention and stability similar to a fixed prosthesis and also better aesthetics and hygiene maintenance similar to conventional removable prosthesis. It further splints the abutment teeth thus providing favourable biomechanics. Only disadvantage being periodic replacement of the clip due to wear of the retention clip as a result of repeated removal and placement of prosthesis. [2] Persic et al. evaluated the effects of various treatment options on aesthetics, chewing efficiency and oral health and stated that precision attachment‑retained RPD showed better treatment options as compared to clasp‑retained RPD.[8]
Most denture wearers are unable to perform satisfactory masticatory functions due to lack of retention of the conventional removable prosthesis. Also in a long distal extension edentulous case, giving a conventional RPD or precision attachment denture do not give satisfactory results. In such cases, cast partial denture is the key for a better retentive prosthesis. Primary retention for such dentures can be achieved by placing retaining elements on the selected abutment teeth, while secondary retention can be achieved through the intimate contact of the underlying tissues with the denture bases and the major connector. Moreover cast circumferential clasps offer greater stability because it has a rigid shoulder.[9] Also cast partial dentures are a better means as compared to conventional dentures in aiding taste sensation of patients due to the ability of transmission of heat.
Conclusion
Although fixed dental prosthesis and dental implants are in trend, conventional RPDs are still prevalent and better opted. The aim should be not only towards restoring oral functions and speech, but also on restoring aesthetics which proper planning and selection of patients. Patient expectations should be taken into consideration before any treatment procedure. Conventional RPDs with specific modifications are yet considered best and gold standard treatment for any partially edentulous individual.
Source of Funding
None.
Conflict of Interest
None.
References
- A B Carr, D T Brown. McCracken’s Removable Partial Prosthodontics. 2011. [Google Scholar]
- VimalKantilal Munot, RameshP Nayakar, Raghunath Patil. Prosthetic rehabilitation of mandibular defects with fixed-removable partial denture prosthesis using precision attachment: A twin case report. Contemp Clin Dent 2017. [Google Scholar]
- R.P. Renner, B.C. Gomes, M.L. Shakun, P.N. Baer, R.K. Davis, P. Camp. Four-year longitudinal study of the periodontal health status of overdenture patients. J Prosthet Dent 1984. [Google Scholar]
- Robert D. Cowan, John A. Gilbert, Dean A. Elledge, F. Dudley McGlynn. Patient use of removable partial dentures: Two- and four-year telephone interviews. J Prosthet Dent 1991. [Google Scholar]
- Göran Agerberg, Gunnar E. Carlsson. Chewing Ability in Relation to Dental and General Health. Acta Odontol Scand 1981. [Google Scholar]
- Krishan K. Kapur, Robert Deupree, Robert J. Dent, Allen L. Hasse. A randomized clinical trial of two basic removable partial denture designs. Part I: Comparisons of five-year success rates and periodontal health. J Prosthet Dent 1994. [Google Scholar]
- RupandeepKaur Samra, ShreenivasVasant Bhide, Chhavi Goyal, Taranjit Kaur. Tooth supported overdenture: A concept overshadowed but not yet forgotten!. J Oral Res Rev 2015. [Google Scholar]
- S Persic, J Kranjcic, D K Pavicic, V L Mikic, A Celebic. Treatment outcomes based on patients’ self‑reported measures after receiving new clasp or precision attachment‑retained removable partial dentures. J Prosthodont 2015. [Google Scholar]
- P Suwal, R Singh, A Ayer, D Roy, R Roy. Cast Partial Denture versus Acrylic Partial Denture for Replacement of Missing Teeth in Partially Edentulous Patients. J of Dent Materials and Techniques 2017. [Google Scholar]
- Introduction
- Case 1: Rehabilitation with tooth supported overdenture
- Case Report
- Case 2: Rehabilitation using precision attachment fixed removable prosthesis
- Case Report
- Case 3: Rehabilitation with a cast partial removable prosthesis
- Case Report
- Discussion
- Conclusion
- Source of Funding
- Conflict of Interest