- Visibility 154 Views
- Downloads 24 Downloads
- Permissions
- DOI 10.18231/j.aprd.2025.016
-
CrossMark

Precision with semi-precision attachment using CAD/CAM technology for a mandibulectomy patient: A case report
- Author Details:
-
 Preeti Thakur *
Preeti Thakur *
-
Annie Cleetus
-
Irfanul Huda
-
Santosh Anand
-
Mohan Kadao
Abstract
Rehabilitation of mandibular defects post-marginal mandibulectomy presents significant challenges due to altered anatomy, reduced denture-bearing areas, and compromised muscle attachments that affect tongue mobility, speech, and mastication. Traditional implant-supported options may be unsuitable for patients with insufficient bone support, necessitating alternative prosthetic approaches to restore function and aesthetics.A 17-year-old male underwent a marginal mandibulectomy for odontogenic keratocyst, resulting in a Cantor and Curtis Type V defect. Examination revealed limited residual dentition and insufficient bone volume for implants. The patient reported difficulties with mastication and speech, requiring a stable, retentive prosthesis that would not exacerbate the altered mandibular anatomy.A removable cast partial denture with semi-precision attachments was fabricated using CAD/CAM technology for accuracy and ease of customization. This approach provided necessary retention, stability, and comfort while accommodating the anatomical limitations. The patient reported significant improvements in mastication, speech, and aesthetics, along with high satisfaction.
Semi-precision attachments offer enhanced stability in cases where conventional direct retainers may be insufficient, distributing occlusal loads effectively across limited supporting structures. CAD/CAM technology facilitated precise attachment placement and minimized chairside adjustments, further improving patient comfort and prosthesis function.For patients with mandibular defects unsuitable for implants, a removable prosthesis with semi-precision attachments, designed with CAD/CAM technology, provides a reliable, conservative alternative. This approach achieves satisfactory functional and aesthetic outcomes, demonstrating the value of modern digital design and attachment-retained prostheses in complex rehabilitative cases.
Introduction
The mandible is a vital structure that forms the lower boundary of the oral cavity and contributes significantly to the facial framework.[1] It works in conjunction with the muscles of mastication and the perioral muscles to shape the lower third of the face, playing a key role in functions such as chewing, speaking, and swallowing. In cases where a marginal mandibulectomy is performed, a portion of the mandible along with the overlying soft tissues is surgically removed. [2] The procedure typically preserves the inferior cortex of the mandible, ensuring the continuity of the lower bone structure.
Anterior mandibular defects pose greater challenges to prosthodontic rehabilitation than posterior defects. This is due to the loss of critical muscle attachments, such as the genioglossus and geniohyoid muscles, which are responsible for controlling the movement of the tongue. These muscles are integral for maintaining proper tongue function, which in turn affects speech, swallowing, mastication, and the ability to control a prosthesis within the oral cavity. The compromised mobility of the tongue resulting from these muscle losses can make it more difficult for the patient to manage food, pronounce words clearly, and maintain stability with removable prosthetic devices. [3]
In addition to the loss of these important muscle attachments, radical alveolectomy—which often accompanies mandibulectomy—results in a significant reduction in the vertical height of the alveolar ridge and the depth of the vestibule. These changes reduce the available soft tissues for support and further challenge the stability of soft-tissue-supported prostheses. [2], [3] With less tissue available to anchor the prosthesis, achieving proper retention and stability becomes more difficult.
This case report presents a comprehensive approach to rehabilitating a patient who has undergone a marginal mandibulectomy and now faces a Cantor and Curtis Type V mandibular defect. The patient was treated using a semi-precision attachment system, which provided both functional and aesthetic restoration of the missing mandibular structures.
Case Description
A 17-year-old male patient ([Figure 1]) was referred to the Department of Prosthodontics and Crown & Bridge for the rehabilitation of a residual defect following mandibulectomy. The patient's medical history indicated that he underwent a marginal mandibulectomy approximately 18 months ago to treat an odontogenic keratocyst.
Upon intraoral examination, the remaining teeth included the right mandibular second premolar and the first and second molars, along with the left mandibular first and second molars ([Figure 2]). The remaining natural teeth showed minimal bleeding upon probing, with no visible caries or mobility.
A panoramic radiograph taken post-surgery revealed that the resection involved the mandibular teeth and alveolar bone, sparing the inferior cortex. The reconstruction plate in place resulted in a continuity defect ([Figure 3]).
The patient exhibited a prognathic facial profile and reported challenges with mastication and speech.
To address the mandibular defect, multiple treatment options were considered:
Fixed dental prosthesis.
Implant-supported prosthesis.
Surgical reconstruction followed by implant-supported prosthesis.
Removable partial denture.
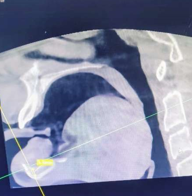
Given that implant-supported prostheses are generally the preferred treatment, a CBCT scan was performed ([Figure 4]) to evaluate the available bone structure. The scan revealed insufficient bone volume for implants, in addition to excessive crown height space. Consequently, the treatment plan was adjusted to restore function and aesthetics using a removable cast partial denture with semi-precision attachments.














Clinical procedure
The treatment plan was carefully explained to the patient, and informed consent was obtained.
Impressions were taken for the mandibular arch using polyvinyl siloxane impression material, while impressions for the maxillary arch were made using irreversible hydrocolloid material ([Figure 5]). These impressions were used to create diagnostic casts, which were analyzed for treatment planning, and a mock-up prosthesis was fabricated.
The mandibular right premolar and first molar were prepared for splinted crowns, and the mandibular left first molar was prepared for a three-unit, single-piece PFM crown with shoulder margins ([Figure 6]).
A final impression was captured using a two-step dual-stage technique with polyvinyl siloxane (putty and light body), followed by beading and boxing ([Figure 7]).
The impressions were cast in Type IV dental stone to produce the working model.
The working model was digitized by scanning ([Figure 8]), and a prosthesis was designed digitally with CAD/CAM technology to ensure precise adaptation ([Figure 9]).
The male components of semi-precision attachments were integrated into the design and positioned on the mesial surfaces of the mandibular left second molar and the mandibular right second premolar. After successful metal framework trials, the PFM crowns were fixed in place using glass ionomer cement ([Figure 10]).
The framework for the partial denture, containing the matrix components, was tried intraorally to verify stability and adaptation ([Figure 11]).
Using the framework as a base, bite registration and jaw relation were recorded. Orientation was performed with a facebow to ensure proper alignment ([Figure 12]).
The teeth were arranged, and the setup was evaluated during a trial phase to confirm aesthetics and occlusal harmony ([Figure 13]).
The partial denture underwent processing, finishing, and polishing to achieve a final, functional prosthesis ([Figure 14]).
The completed cast partial denture, incorporating the semi-precision attachments, was delivered and inserted into the patient’s mouth. Detailed instructions for maintenance and care were provided ([Figure 15]).
During the insertion appointment, the prosthesis was evaluated for fit, stability, and functionality.
A follow-up was scheduled after one week, during which minor adjustments were made to improve comfort and ensure the prosthesis met the patient's needs.
Discussion
Prosthodontic rehabilitation for mandibular defects involves addressing complex challenges, such as insufficient denture-bearing areas, altered floor-of-mouth anatomy, and limited remaining teeth with compromised periodontal health. Psychological factors also play a role in patient hesitation toward invasive treatments. Many patients avoid surgical options due to prolonged healing times and existing discomfort, which impacts their willingness to undergo procedures like implant placement or pre-prosthetic surgeries. These considerations can limit prosthesis design, retention, and stability.[4]
To optimize partial denture retention and stability, advanced methods such as the use of multiple abutments and semi-precision attachments are often employed. These attachments, combined with direct retainers, enhance the prosthesis's retention and functional effectiveness. [5]
Fabrication of prostheses incorporating extracoronal semi-precision attachments is highly technique-sensitive. Precision is required for aligning attachments parallelly to ensure proper prosthetic seating and functionality. Additionally, the duplication of master casts and framework fabrication necessitates a meticulous approach to achieve the desired outcome. [6]
In this case, semi-precision attachments were employed to improve retention and to allow controlled prosthetic movement, ensuring even distribution of functional forces across the supporting structures. This strategy enhanced the prosthesis's stability while maintaining long-term usability. The resulting prosthesis restored essential functions such as mastication and speech and improved aesthetics by providing lip support in the mandibular anterior region. [7]
Semi-precision attachments provide several advantages in mandibular defect rehabilitation. They improve retention, distribute functional forces more effectively, and reduce the stress on abutment teeth. Their extra coronal design permits minor movement of the prosthesis, contributing to durability and comfort. Furthermore, they are aesthetically advantageous, as they minimize visible metal compared to conventional direct retainers. However, their design and fabrication require precise planning and execution to ensure accurate fit and alignment.
The integration of CAD/CAM technology has further revolutionized prosthetic rehabilitation, offering unparalleled accuracy and customization. Digital workflows facilitated the design of the semi-precision attachments and frameworks in this case, ensuring precise alignment and fit. The CAD/CAM process encompasses three stages: [8]
Digital Impression: The dental anatomy is captured using optical scanning technology to create an accurate digital model.
CAD Design: Using computer-aided design software, the restoration is digitally planned to ensure optimal fit, retention, and aesthetic appeal.
CAM Fabrication: The design is then fabricated using milling machines or 3D printing, resulting in a high-precision prosthesis tailored to the patient's anatomy.
This approach minimized the need for chairside adjustments and allowed for long-term adaptability to changes in the patient's oral condition. The use of semi-precision attachments combined with CAD/CAM technology delivered a stable, functional, and aesthetically pleasing prosthesis, which significantly improved the patient’s confidence and quality of life.
Conclusion
In cases of mandibular defects, attachment-retained removable prostheses fabricated using CAD/CAM technology provide an excellent balance of function and aesthetics without the need for invasive interventions. This approach offers a practical and efficient solution, particularly for patients unsuitable for implant-based restorations. By integrating semi-precision attachments with advanced digital workflows, prosthodontists can achieve durable, retentive, and highly satisfactory outcomes.
Source of Funding
None.
Conflict of Interest
None.
References
- Beumer I, Marunick M, Esposito S. . Maxillofacial Rehabilitation: Prosthodontic and Surgical Management of Cancer-Related, Acquired, and Congenital Defects of the Head and Neck. 2011. [Google Scholar]
- Jacob R, TT. . Prosthodontic rehabilitation of mandibulectomy patient Clinical Maxillofacial Prosthetics. 2000. [Google Scholar]
- Taylor D, Taylor D. Diagnostic considerations for prosthodontics rehabilitation of the mandibulectomy patient. Clinical Maxillofacial Prosthetics. 2000. [Google Scholar]
- Patil P. Conventional complete denture for a left segmental mandibulectomy patient: a clinical report. J Prosthodont Res. 2010;54(4):192-7. [Google Scholar]
- Zhao J, Wang X. Dental prostheses. Advanced ceramics for dentistry . 2014. [Google Scholar]
- Mundhe K, Pruthi G, Jain V. Prosthodontic rehabilitation of patient with marginal mandibular resection using attachment supported prostheses: A clinical report. Contemp Clin Dent. 2014;5(1):123-6. [Google Scholar]
- Khanam H, Bharathi M, Reddy K, Reddy S. Attachments in prosthodontics: different systems of classification: A review. J Evol Med Dent Sci. 2014;14(28). [Google Scholar]
- Maiti N, Mahapatra N, Patel D, Chanchad J, Shah A, Rahaman S. Application of CAD-CAM in Dentistry. Bioinformation. 2024;20(5):547-50. [Google Scholar]